
Authored by Ashitha Abdul Ashraf, Senior Consultant Physiotherapist – Incharge | Medically Reviewed by Dilshana Thasni T, Senior Consultant Physiotherapist | Last Reviewed: June 2026

Neck pain is the second most common musculoskeletal complaint in Kerala after lower back pain. A significant proportion of people over 40 who present with chronic neck pain have some degree of cervical spondylosis — wear and tear changes in the cervical spine that show up on X-ray or MRI.
The good news is that cervical spondylosis sounds worse than it usually is. Most people with spondylosis changes on imaging have manageable symptoms or no symptoms at all. The structural finding on a scan does not determine your outcome. How the condition is treated does.
This guide covers what cervical spondylosis is, what causes it, how it differs from other neck pain, and what non-surgical treatment options are available in Kerala.
What Is Cervical Spondylosis?
Cervical spondylosis is a general term for age-related degeneration of the cervical spine — the seven vertebrae of the neck. It encompasses several related changes that develop over time:
Disc degeneration. Cervical discs lose water content and height as they age. The space between vertebrae narrows. This reduces the cushioning between vertebral bodies and can allow bone-to-bone contact under load.
Osteophyte formation. Bone spurs — called osteophytes — develop at the edges of vertebral bodies in response to increased mechanical stress. These are the body’s attempt to stabilise a degenerating joint. They can narrow the space available for nerve roots exiting the spinal canal.
Facet joint degeneration. The facet joints between vertebrae develop osteoarthritic changes — cartilage thinning, joint space narrowing, and reactive bone formation.
Ligament thickening. The ligamentum flavum — a ligament inside the spinal canal — can thicken over time, further reducing the space available for the spinal cord and nerve roots.
Individually, each of these changes is a normal part of ageing. MRI studies of people in their 40s and 50s with no neck pain consistently show degenerative changes. The clinical problem arises when these changes compress a nerve root or the spinal cord itself — producing symptoms beyond simple neck stiffness and pain.
Cervical Spondylosis vs Other Neck Pain
Not all neck pain is cervical spondylosis. Understanding the difference affects treatment.
Muscle tension neck pain is the most common type in younger adults and desk workers. It is driven by postural overload, stress, and sustained static positioning. There are no structural changes on imaging. It responds quickly to physiotherapy, postural correction, and stress management.
Cervical disc herniation is a distinct condition from spondylosis, though they can coexist. A disc herniation involves the inner disc material pushing through a tear in the outer ring — pressing directly on a nerve root. It causes more acute, often more severe symptoms than spondylosis-related nerve compression.
Cervical spondylotic radiculopathy is spondylosis that has compressed a nerve root — causing arm pain, numbness, or weakness. This is where spondylosis crosses from a background structural finding to a clinically significant condition requiring targeted treatment.
Cervical spondylotic myelopathy is compression of the spinal cord itself by spondylotic changes. This is the most serious presentation — causing progressive weakness, coordination problems, and sensory changes in the limbs and trunk. It requires urgent specialist assessment and often surgical intervention.
Symptoms: What Cervical Spondylosis Feels Like
Symptoms vary depending on whether the spondylotic changes are compressing nerve roots, the spinal cord, or neither.
Without nerve compression (axial neck pain):
- Neck stiffness, particularly in the morning
- Aching in the neck and upper shoulders
- Reduced range of motion — difficulty turning the head fully
- Headaches arising from the base of the skull
- Symptoms that worsen with sustained postures — looking down at a phone, reading, driving
With nerve root compression (radiculopathy):
- Pain that radiates from the neck into the shoulder, arm, or hand
- Numbness or tingling in specific fingers — the distribution depends on which nerve root is compressed
- Weakness in specific arm or hand muscles
- Symptoms that worsen with neck extension or lateral bending toward the affected side
- Relief when the arm is raised above the head — a classic sign of cervical radiculopathy
With spinal cord compression (myelopathy):
- Progressive weakness or clumsiness in the hands — difficulty with fine motor tasks like buttoning, writing
- Unsteady walking or balance problems
- Sensation of electric shock running down the spine when the neck is bent forward (Lhermitte’s sign)
- Bladder or bowel dysfunction in severe cases
Myelopathy symptoms require urgent neurological or spinal surgical assessment. Do not wait for physiotherapy if you have these features.
How Cervical Spondylosis Is Diagnosed
A combination of clinical assessment and imaging confirms the diagnosis and determines the appropriate treatment.
Clinical assessment. A physiotherapist or doctor will assess your neck range of motion, neurological function in the arms — reflexes, sensation, muscle strength — and perform specific clinical tests for nerve root and spinal cord involvement. The clinical picture determines whether imaging is needed and what type.
X-ray. Shows bony changes — disc space narrowing, osteophytes, alignment. The first-line imaging for cervical spondylosis assessment.
MRI. Shows soft tissue in detail — disc condition, nerve root compression, spinal cord compression, ligament changes. Needed when radiculopathy or myelopathy is suspected. MRI findings must always be interpreted alongside clinical examination — spondylotic changes on MRI without matching clinical symptoms are not automatically a treatment indication.
Nerve conduction studies. Occasionally needed to confirm the level of nerve involvement when clinical and imaging findings are inconsistent.
Non-Surgical Treatment for Cervical Spondylosis
The vast majority of cervical spondylosis — including cases with radiculopathy — is managed successfully without surgery. A genuine trial of conservative treatment is appropriate for all cases except progressive myelopathy or severe neurological deficit.
Physiotherapy and Manual Therapy
The foundation of conservative cervical spondylosis management.
Joint mobilisation. Gentle, specific movement of stiff cervical joints restores range of motion, reduces pain, and improves function. For cervical spondylosis with axial neck pain and stiffness, manual therapy is one of the most effective interventions available. Multiple randomised controlled trials show cervical joint mobilisation produces better short and medium-term outcomes than medication or rest alone.
Deep neck flexor strengthening. The deep cervical flexors — longus colli and longus capitis — are the primary stabilisers of the cervical spine. They are consistently weak and inhibited in people with cervical spondylosis and chronic neck pain. Strengthening these muscles reduces cervical spine loading and improves posture.
Postural retraining. Correcting forward head posture reduces the mechanical load on spondylotic cervical segments. A head held 7 to 8 cm forward of neutral dramatically increases the load on the cervical spine. Postural correction is not a short-term fix — it requires consistent practice over months to change established patterns.
Neural mobilisation. For radiculopathy cases, gentle nerve mobilisation exercises — sliding and tensioning movements that restore the nerve’s ability to move freely through surrounding tissue — reduce neural sensitivity and arm symptoms.
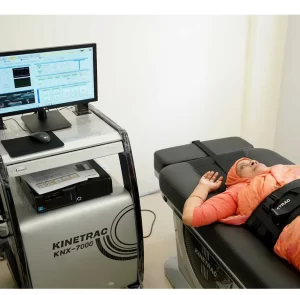
Cervical Spinal Decompression
For cervical spondylosis with significant radiculopathy — arm pain, numbness, or weakness from nerve root compression — cervical spinal decompression is the most targeted non-surgical treatment available.
The KNX-7000 system applies precise, controlled traction to the cervical spine at a specific angle calculated for your disc and nerve level. This creates negative intradiscal pressure that reduces nerve root compression and promotes disc rehydration.
For patients with cervical radiculopathy that has not responded adequately to manual therapy and exercise, cervical spinal decompression often produces the improvement that other conservative measures cannot achieve. A typical course is 10 to 15 sessions.
This is available at Maana Health clinics across Kerala.
Exercise Therapy
A progressive exercise program for cervical spondylosis addresses muscle imbalances, improves cervical and thoracic mobility, and builds the endurance of the muscles that support the neck throughout the working day.
Key exercises include deep neck flexor activation (chin tucks), scapular stabilisation, thoracic extension, and progressive cervical strengthening in pain-free ranges. These are prescribed specifically for your deficit pattern — not a generic neck exercise sheet.
Electrotherapy
TENS provides symptomatic pain relief, particularly for acute flare-ups of cervical spondylosis. Therapeutic ultrasound reduces local soft tissue inflammation. These are supportive treatments — they manage symptoms while the primary structural treatment — manual therapy, exercise, decompression — addresses the underlying cause.
Lifestyle and Ergonomic Modification
For desk workers with cervical spondylosis — the majority of cases in Kerala’s working population — ergonomic correction is a required component of treatment, not an optional add-on.
Screen at eye level. This single change reduces the sustained cervical load that is the primary driver of spondylosis progression in desk workers. Laptop users need a stand and separate keyboard.
Phone use posture. Looking down at a mobile phone held in the lap produces sustained cervical flexion load equivalent to carrying 20 to 27 kg on the neck for the duration of that use. Hold the phone higher.
Pillow height. A pillow that holds the cervical spine in a neutral position during sleep matters. Too high or too low both produce hours of sustained cervical loading at night.
When Surgery Is Considered
Surgery for cervical spondylosis is appropriate in specific situations.
Progressive myelopathy. Spinal cord compression that is causing progressive neurological deterioration — worsening hand weakness, balance problems, bladder involvement — requires surgical decompression. Physiotherapy cannot reverse spinal cord compression from significant structural stenosis.
Severe radiculopathy with progressive neurological deficit. If arm weakness is worsening despite conservative treatment, or if neurological signs are severe at presentation, surgical decompression of the nerve root is appropriate.
Failed conservative treatment for radiculopathy. If a genuine 12-week trial of targeted physiotherapy, including cervical decompression where appropriate, has not produced adequate improvement in arm symptoms, surgical consultation is reasonable.
For axial neck pain — pain without significant nerve involvement — surgery is very rarely appropriate regardless of the degree of spondylotic change on imaging.
Frequently Asked Questions
Does cervical spondylosis get worse over time?
Structurally, some progression is normal as part of ageing. Clinically, many people with spondylotic changes on imaging remain symptom-free or have manageable symptoms for years with appropriate physiotherapy and lifestyle management. Progression to significant radiculopathy or myelopathy is not inevitable.
Can physiotherapy reverse cervical spondylosis?
Physiotherapy cannot reverse the structural changes of spondylosis — disc degeneration and osteophytes do not disappear with treatment. What physiotherapy does is reduce symptoms, improve function, strengthen the muscles that protect the cervical spine, and correct the postural and movement patterns that accelerate spondylotic progression.
Is it safe to have my neck manipulated with cervical spondylosis?
Gentle cervical joint mobilisation — the technique used in physiotherapy — is safe for most cervical spondylosis cases. High-velocity manipulation (the type used in some chiropractic treatment) carries a small but real risk in the presence of significant spondylotic changes. At Maana Health, cervical treatment is assessed and delivered specifically for your degree of spondylosis.
My X-ray shows bone spurs. Do they need to be removed?
Rarely. Bone spurs on X-ray are not a surgical indication on their own. Surgery is considered only when bone spurs are compressing a nerve root or the spinal cord and producing significant neurological symptoms that have not responded to conservative treatment.
How long does physiotherapy take for cervical spondylosis?
For axial neck pain without nerve involvement, 6 to 10 sessions typically produces significant improvement. For radiculopathy, 12 to 20 sessions including cervical decompression is a reasonable course before reassessment. Maintenance physiotherapy and ongoing exercise are beneficial for long-term management.
Maana Health treats cervical spondylosis and neck pain across five clinics in Kerala — Kochi, Calicut, Perinthalmanna, Aluva, and Trivandrum. If you have chronic neck pain, arm symptoms, or have been told your MRI shows spondylotic changes, book a free assessment and get a clear picture of your treatment options.